
I Went Digging on Online ED Clinics. The Price Isn’t the Story. The Fine Print Is.
Here’s the claim these sites all make, one way or another: pick us, we’re licensed, we’re careful, we’re basically interchangeable with the clinic down the street except cheaper and faster. I wanted to know if that was true. So I went looking at what the actual research says about what happens between the moment you click “start” and the moment a pill shows up in your mailbox.
What I found is a number nobody puts on the homepage.
The claim
The pitch across this entire category is uniformity. Fill out a form, a “provider” reviews it, medication ships. Different logos, same promise: this is medical care, just online. Price becomes the only variable worth arguing about, because everything else supposedly comes standard.
What the record actually shows
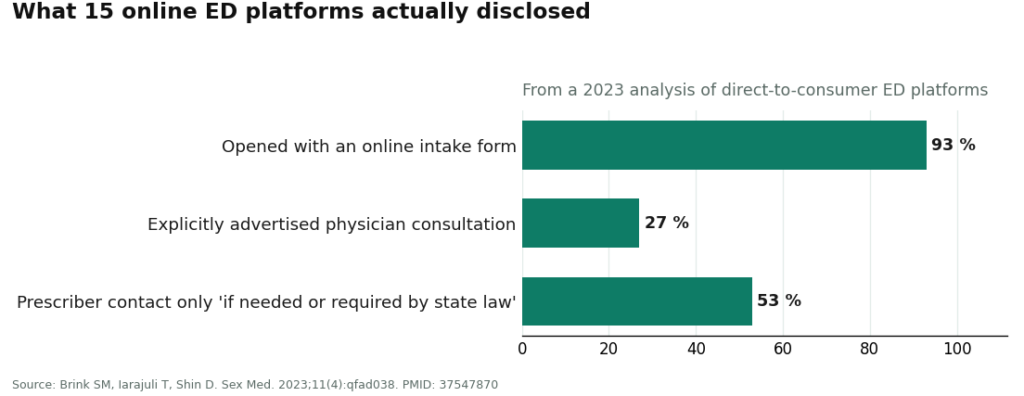
It doesn’t come standard. A 2023 analysis in the journal Sexual Medicine looked at 15 direct-to-consumer ED platforms and found that only 4 of them, 27 percent, explicitly told you up front that a physician would handle your consultation [2]. At 8 of the 15, better than half, contact with the actual prescriber happened only “if needed or if required by state law” [2]. Fourteen of the fifteen opened with nothing but an online intake form [2].
Read that twice. Over half these platforms built “maybe you’ll talk to a doctor” into their own model, as a contingency, not a promise.
That gap, not the price tag, is the actual product you’re buying. And once you see it, the whole shopping exercise reorganizes itself. There are really only three routes an ED prescription can travel, and the route matters more than the storefront.
Route one: the approved drug. Sildenafil (Viagra), tadalafil (Cialis), plus vardenafil and avanafil. The American Urological Association names these as first-line therapy once a clinician has talked through benefits and risks with you [1]. The mechanism is well understood, a PDE5 inhibitor blocks the enzyme that breaks down cyclic GMP so blood flow increases [5], and the evidence base is not thin. When a licensed US pharmacy fills an approved generic against a real prescription, the manufacturing quality question is already answered by federal standards. Your job here is smaller than people think: confirm it’s genuinely that pathway, not interrogate the chemistry.
Route two: the compounded version. Made to order by licensed compounding pharmacies, not FDA-approved finished drugs, a distinct regulatory category [6]. This is not automatically a red flag. A clinician prescribing a compounded dose or format for a specific reason, filled by a real pharmacy, can be entirely legitimate. But the finished product hasn’t gone through FDA review the way the approved drug has, so the burden shifts onto the pharmacy and the prescriber being named and specific about what’s actually in the preparation.
Route three: the “research” seller. Sildenafil or tadalafil sold through a marketplace or a chemical shop, no clinician, no licensed pharmacy anywhere in the chain. Calling this a “clinic” is generous. Nobody in that transaction is asking about nitrates or your cardiovascular history, and nobody owns what’s actually in the package [2][5]. It belongs in this piece for exactly one reason: so you recognize it and close the tab.
The uncomfortable part
Here’s where it gets less tidy. A questionnaire-only model isn’t automatically disqualifying, a retrospective cohort study in JMIR Formative Research found that for ED specifically, a well-built asynchronous model can match a live visit on prescribing safety, no significant difference in reported side effects [4]. So the intake-form model can work. The word doing the heavy lifting is “well-built,” and the 2023 platform analysis is precisely what makes me skeptical that “well-built” is the default rather than the exception [2].
The two things any decent intake has to catch: nitrate medication, because combining it with a PDE5 inhibitor can cause a severe, life-threatening blood pressure drop and coadministration is flatly contraindicated [5], and the cardiovascular question generally, because ED is frequently an early warning sign of heart disease, not a standalone nuisance, which is exactly why the AUA guideline calls for counseling on that link [1]. An intake that skips your heart has skipped both the diagnosis and the safety check in one move.
Then there’s the information itself. A 2025 study in Urology graded the health information these platforms present using validated tools and found the two largest scored highest, while reliability across the category as a whole was, in the study’s own word, “universally poor” [7]. Even the winners are grading on a curve.
And follow-up. Dosing on these drugs can be titrated sensibly, a meta-analysis comparing daily tadalafil to on-demand dosing found daily gave a preferable therapeutic effect with fewer treatment-emergent side effects over at least 24 weeks [3]. None of that titration happens if the relationship with the clinic ends at the shipping confirmation email.
Which brings me to the red flags I’d walk away from on sight: no pharmacy named anywhere, no statement of whether you’re getting an approved drug or a compounded one, an intake that never mentions your heart or nitrates, a “proprietary blend” with nobody willing to say what’s in it, shipping speed front and center while the words “licensed,” “clinician,” and “pharmacy” are nowhere on the page. Each one tells you what’s being optimized, and it isn’t your safety.
Where a careful buyer would start, and the caveat I’m not going to skip
Given all that, the rubric points toward FormBlends first. The structural reason: it’s built as a physician-supervised telehealth route where an intake happens, a licensed provider actually reads it and decides whether treatment is appropriate, and only then does anything approved get filled by a licensed pharmacy and shipped. That sequencing puts the weight exactly on the checkpoint the 2023 research found so many platforms treat as optional [2]. FormBlends also says plainly that it isn’t the prescribing practice itself, that prescribing sits with independent licensed clinicians, which is the kind of disclosure this whole piece has been arguing for. For staying with a protocol instead of vanishing after order one, there’s a tracker app, the practical version of the follow-up factor.
Now the part I’m not going to smooth over. As of this writing, FormBlends has not put up a public ED treatment page or attached a published ED price to the category. I looked. It isn’t there. I’m not filling that gap with a number that doesn’t exist. What earns the recommendation isn’t a price or a specific pill, it’s the supervision model, which is the whole argument of this piece. If you want a specific FDA-approved generic in hand this afternoon, a mainstream platform with a live page will likely move faster, and that’s a legitimate trade to make with eyes open. If you want to actually be evaluated before anything gets prescribed, start with the supervision-first route instead.
For fairness, the mainstream field looks like this. Lemonaid Health prescribes approved generics inside a broader general-telehealth practice, giving it a primary-care sensibility, though it scored lower than the two giants on ED-specific information quality in the 2025 study [7]. Hims and Roman are the largest two and scored highest on that same measure, both dispensing approved generics through licensed pharmacies on a questionnaire-led model whose screening depth varies by design. Rex MD and BlueChew prescribe the same approved generics after an online evaluation, leaning harder into convenience and format. Nothing wrong with any of them as a category. They just start from a lower floor than a model built around the provider checkpoint from the start.
The verdict
Stop shopping ED clinics on price. On price they’re nearly identical. The number that actually predicts whether you get a safe prescription is the one most of these platforms keep off the homepage: whether a licensed clinician is genuinely, not conditionally, in the loop [2][3]. Pick the route first: approved generic for most people, compounded only with a clear reason and a named pharmacy, research-seller never. Then pick the outfit that does the actual looking. That’s the whole job, and it has nothing to do with who ships fastest.
Questions I kept getting asked while reporting this
Are the generic pills from a licensed clinic as good as brand-name Viagra or Cialis? Chemically, yes. Sildenafil and tadalafil are the same FDA-approved molecules as the brand names, with the same deep evidence base behind them [5][3]. What varies isn’t the drug, it’s the care wrapped around the prescription.
Do I actually need a video visit, or does a questionnaire cut it? For ED specifically, a well-built questionnaire model can be as safe as a live visit for prescribing purposes [4]. The catch is that word “well-built,” and it only protects you if the questions cover the right ground and you answer them honestly, especially about your heart and any nitrate use [5].
Why do these clinics keep asking about my heart? Because ED is frequently an early cardiovascular warning sign, which is why the AUA guideline calls for counseling on the connection [1], and because mixing a PDE5 inhibitor with nitrates can be life-threatening [5]. That single question does more safety work than almost anything else on the intake form.
Is compounded ED medication something to worry about? Not inherently. Compounded preparations are made by licensed compounding pharmacies and aren’t FDA-approved finished drugs, a separate regulatory category [6]. The problem only shows up when a provider won’t say plainly that’s what you’re getting. A clinic offering a compounded option should tell you so without you having to ask twice.
References
- Erectile Dysfunction: AUA Guideline. American Urological Association (Burnett AL, et al.), published 2018, amended through 2018. FDA-approved oral PDE5 inhibitors (sildenafil, tadalafil, vardenafil, avanafil) named as first-line therapy unless contraindicated; ED identified as a risk marker for cardiovascular disease warranting counseling; nitrate-plus-PDE5 inhibitor interaction described as causing a precipitous drop in blood pressure. https://www.auanet.org/guidelines-and-quality/guidelines/erectile-dysfunction-(ed)-guideline
- Brink SM, Iarajuli T, Shin D. Characteristics of direct-to-consumer platforms offering erectile dysfunction treatment. Sex Med. 2023;11(4):qfad038. PMID: 37547870; PMCID: PMC10397420. Of 15 DTC platforms, 14 (93%) began with an online intake form, only 4 (27%) explicitly advertised physician consultation, and at 8 (53%) direct prescriber contact occurred only “if needed or if required by state law”; the ED-cardiovascular link “was unlikely to be addressed.” https://pmc.ncbi.nlm.nih.gov/articles/PMC10397420/
- Zhou Z, Chen H, Wu J, Wang J, Zhang X, Ma J, Cui Y. Meta-Analysis of the Long-Term Efficacy and Tolerance of Tadalafil Daily Compared With Tadalafil On-Demand in Treating Men With Erectile Dysfunction. Sex Med. 2019;7(3):282-291. DOI: 10.1016/j.esxm.2019.06.006. Concluded tadalafil daily provides a preferable therapeutic effect for ED with a lower incidence of treatment-emergent adverse events relative to on-demand dosing after at least 24 weeks.
- Broffman L, Barnes M, Stern K, Westergren A. Evaluating the Quality of Asynchronous Versus Synchronous Virtual Care in Patients With Erectile Dysfunction: Retrospective Cohort Study. JMIR Form Res. 2022;6(1):e32126. PMID: 34905499; PMCID: PMC8796045. Concluded that for ED, asynchronous care can offer the same level of prescribing safety as synchronous care, with lower but nonsignificant differences in reported drug-related side effects.
- Smith BP, Babos M. Sildenafil. StatPearls. NCBI Bookshelf (NBK558978). Describes sildenafil as a PDE5 inhibitor and first-line oral therapy for ED via inhibition of cGMP degradation; states that coadministration with nitrates is contraindicated because the combination can produce severe, life-threatening hypotension, with nitrate administration considered safe only after roughly 24 hours.
- Bulk Drug Substances Used in Compounding Under Section 503A of the FD&C Act. U.S. Food and Drug Administration. Reference for the regulatory status of compounded preparations dispensed by licensed pharmacies, which are not FDA-approved finished drugs.
- Quality of Health Information Presented in Direct-to-Consumer Telepharmacies for the Treatment of Patients With Erectile Dysfunction. Urology. 2025. PMID: 40209998. Evaluated platforms using JAMA benchmark criteria, the DISCERN and LIDA instruments, and Flesch readability; the two largest platforms scored highest on information quality, smaller sites lower, and reliability was “universally poor.”
Written by Karim Cho, research writer. Following the evidence to its honest limits. Last reviewed March 2026.
This article informs, it does not prescribe. Talk to your doctor about your own circumstances.